I think there is a fundamental misunderstanding as to what is meant as the hospitals are being overwhelmed. It is correct that on a whole some hospitals may not have their beds filled, and in many hospitals there have been significant layoffs of nurses and personnel for many medical areas which were not considered essential treatment. Hospitals are very restrictive as far as doing elective or non-critical treatments, so yes many of the hospitals may appear as being empty on certain wards. Treatment of covid patients requires a negative pressure rooms which are very uncommon, the 300 bed hospital that I worked at had 2 such rooms at the time, shortly after the epidemic they retrofitted one ward (about 30 beds) to negative pressure rooms and also sealed to address covid infected patients. You need respirators, monitoring equipment, etc. In addition there is a requirement of a fixed critical care nursing staffing ratio, with nurses qualified (and willing) to take care of critical care covid patients and the equipment required to treat these patients. Many of these patients are triaged to tertiary medical centers that are equipped to treat these patients, and as such, many smaller hospitals have very low occupancy and many may not survive due to loss revenue. So lets put this all in context, hospitals are so restrictive as to who comes in, that I recently had a surgical procedure and the surgeon had to do it at a stand alone surgery center as opposed to admitting me to a hospital.
One also need to take into account the hot spots and the epidemiology of the outbreaks, it is a fact that in the hot spots the hospitals are running at capacity to treat covid patients, many now are triaging covid patients to other hospitals with the capacity to treat these patients in a dedicated rooms/wards. So if you show up at the hospital with covid say you are 75 with preexisting conditions and next to you is another patient who is 45 in good health otherwise who do you think will get treated first and more aggressively. My mom who lives in Phoenix is 91 in great health, was pretty much told by her medical doctor that when the hospitals are beyond capacity, pretty much if you are over 75 and/or have co-morbid conditions you are pretty much toast. If you recall in New York when the covid cases were spiking and they had no more beds, they were lining up the bodies like cord wood in refrigerated tractor trailers. We have far surpassed those numbers seen in the first wave and we are now seeing more than 2000 deaths per day with the beginning of this second wave. In the next "month" more people will die from covid, then the worst year then those who succumbed to the seasonal flu. This is not a bad case of the flu, it is not going to go away anytime soon, and the daily cases/death toll will continue to climb at an alarming rate in the next several months. Unfortunately by the time a vaccine rolls out and people receive there 2 doses, we will probably see a doubling of the current death toll without draconian measures which I do not expect to see happen in the US. The UK and the EU have taken a different perspective and they are in a complete lock down mode. With regard to the video statements by Dr. Roger Hodkinson posted by Cooter above, the statements that covid is no worse than a bad case of the flu, he has provided no evidence to substantiate his statements. He lied about his credentials and he is part of a legal medical firm that does medical litigation, so no doubt he will reap a significant amount of notoriety and money from future litigation.
Updated: Clarification on statements made regarding COVID-19 by a Royal College Fellow, Dr. Rodger Hodkinson.

newsroom.royalcollege.ca
The other aspect people are missing is the long term medical complications being seen with covid, we are now understanding that there are are many long-term complications that may not heal with time. The covid treatment options are still very limited and you would be lucky to be treated at a hospital that has a full arsenal of treatment options. At some point, similar to when we call a code on a patient who's heart has stopped, it is all about assessing the medical situation and chance of resuscitation/future survival.
People that site a particular incident or observation is not backed up by data or the facts, is just an observation with no substance or for that matter knowledge. Too many people want to believe what they want and will go to any means to perpetuate their point of view. I have been a medical research investigator on 100's of medical trials to prove or disprove a treatment hypothesis, the studies are designed to try to eliminate bias or any preconceived idea's, one reason why they are called double blind studies. I have seen countless testimonials in the treatment of cancer during my medical career such as high dose vit. C, laetrile, and all sort of other magic bullets only to be disproved in randomized clinical trials.
With regard to heard immunity and reinfection, there are documented cases of reinfection based on genetic mapping of the virus, to what degree this occurs is unknown and to some degree many individuals may be silent carriers for a period of time while unknowingly infecting others. It would appear that the degree that this occurs and the viral load may be diminished because of prior exposure. Risk and severity of covid infection appears to be dependent on the quantity of virus transmitter to another person, so acute high level or longer continuous exposure all seem to be factors. This may be one reason why masks and social distancing have appeared to make an impact in propagation of the virus. So it is not that you are blocking 100% of the virus, but your are diminishing the quantity, and as such your body has more time to mount an immune response. On the issue of why should I wear a mask, there is now an abundance of information that states/areas that have mandated these measures that control of covid transmission is reduced vs. increased. There has also been a massive reduction in covid transmission in many Asian countries with the requirement of mask wearing and better sanitation such as hand disinfection. This may not only be due to mask wearing, but additional measures to limit social contact. If you feel this is a restriction of freedom of individual expression, then why do we have laws that limit how you drive and treat other people. If you get TB, you must wear a mask to protect other, we know this works. QED.
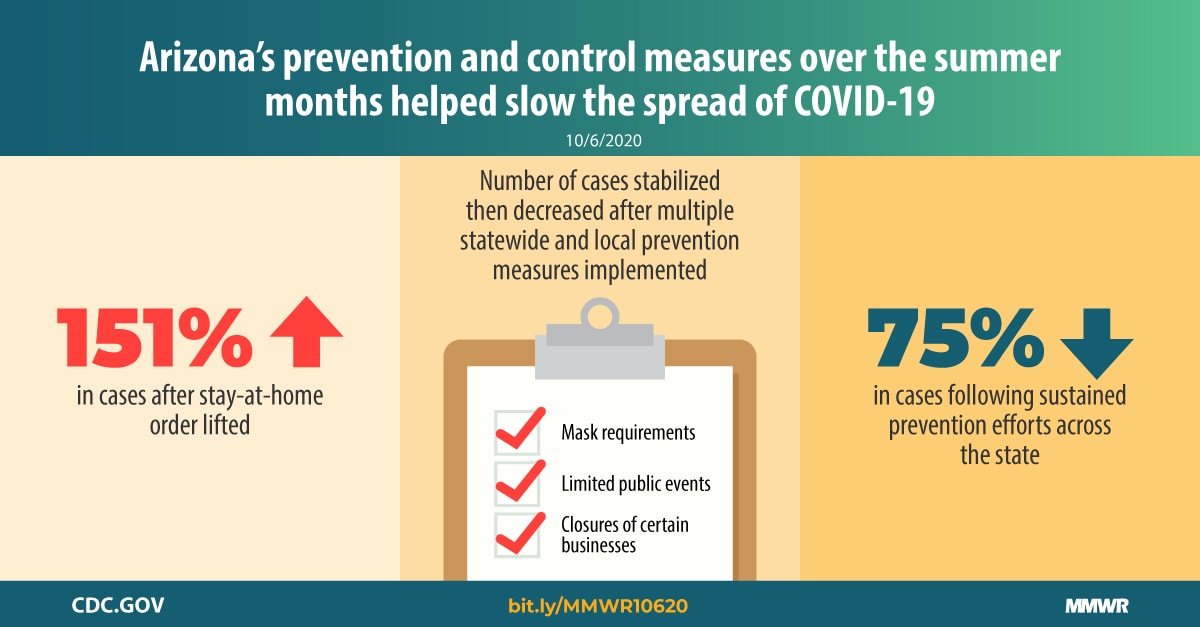
This report describes trends in the number of COVID-19 cases in Arizona after sustained implementation and enforcement of statewide and locally enhanced mitigation measures.

www.cdc.gov
We are in difficult times, we need a consensus and direction, we are all in this together. If we do not look at the facts and make hard choices, some of which we may not all agree on, things are going to get much worse. I have my concerns about the covid vaccines, but the data so far is encouraging enough that it could save millions of lives and will only be effective if we hit a certain threshold of people vaccinated. Individuals having had prior covid may benefit from the vaccine to help prevent different variants of future infection, this is seen with individuals that have had previous Herpes Zoster and are still recommended by the CDC to get Shingrix which is a recombinant (synthesized) DNA vaccine. The major Covid vaccines are recombinant RNA, this vaccine technology is also in other clinical trials for many other indocations such as HPV and cancer indications.
I will not be adding any further comments to this thread, we all need to look at the facts and make rational choices for the future of humanity.